About the case study:
The role of local nurse and National Nursing Association, in disaster management after the devastating earthquake in April 25, 2015 shows how nurses supported a technological innovation in managing health information in the country during and after the disaster. Nurses were trained on rapid health assessment and use of open source mapping and referral system and a surveillance system to help in gathering information on the ground to inform health interventions. This result shows one of the ways practical and solution oriented research can challenge the conventional public health security monitoring systems which require near real-time, population-based, statistical alarms to alert to unusual activity. The potential of this collaboration is not only to produce innovative research outcomes involving the improvement or optimization of services utilizing ICT, but also to promote research knowledge and idea exchange regarding social issues and challenges in the field of emergency preparedness and response.
Reference Paper:Kanbara Sakiko (2016): Participatory Surveillance on evacuation site by local nurses and ICT in Nepal in Shaw R., Izumi T., Shi P., Lu L., Yang S., Ye Q. (2016): Asia Science Technology Status for Disaster Risk Reduction, published by IRDR, Future Earth and ASTAAG, Beijing, China, p. 83
Introduction
Nepal is situated in one of the most seismically active regions of the world. Historical data show that it has experienced a number of devastating earthquakes. Nepal earthquake, also known as the Gorkha earthquake killed over 8,600 people and affected more than 5.6 million individuals; with damage estimates exceeding 3.9 billion US dollars (CRED, 2015). The affected areas include densely populated regions of greater Kathmandu as well as mountainous areas in which rural populations are dispersed. The Ministry of Health and Population in Nepal identified 14 districts severely affected: Gorkha, Dhading, Rasuwa, Sindhupalchok, Kavre, Nuwakot, Dolakha, Kathmandu, Lalitpur, Bhaktapur, Ramechhap, Sindhuli, Okhaldhungai and Makwanpu districts; including Dolakha and Sindhupalchok which were severely affected by the second earthquake (WHO Nepal, 2015).
Problem
Initial public health concerns were caring for the survivors with wounds and injuries; majority with minor cuts and bruises, fractures and with some number requiring surgery and blood transfusion. Provision of emergency medical and surgical cares was an immediate priority including giving tetanus vaccination to patients. Communicable and infectious diseases related to water, sanitation and hygiene were also priorities after the earthquake given the reduced access to safe water and sanitation systems and damaged sewage infrastructures. Other endemic communicable diseases such as Hepatitis and Cholera and diseases associated with overcrowding such as Measles, Diphtheria, Pertussis and Acute Respiratory Infections were all major concerns. Priority interventions for the control and management of communicable diseases include provision of safe drinking water, shelter and site planning, surveillance and early warning and response system, immunization, standard treatment, and public health communication (WHO Nepal, 2015).
Approach / Stakeholder participation
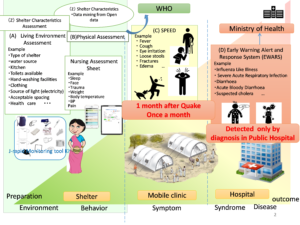
Two days after the earthquake, an immediate concern was how to care for people in the open field and how to reach out to populations in need. One crucial factor was how to get information to help communities recover from the impact of the earthquake and prevent possible epidemics. NAN also continue monitoring with Global collaborated research team funded by Japan Science Technology so that reached out to NAN to help set up information systems to make rapid health assessment and gather more information to prevent outbreaks. To collaborate in real time with Nepali nurses who conduct the surveillance, the Tool kit is customized for health coordination mechanism/development by incorporating the WHO guidelines and application. The most critical challenge is data collection to generate reasonable information that can be used in predicting whether something is likely to occur. Our interest lies in collecting information on the items from the view of public health and nursing including culture, lifestyle and perception. It is developed as an open tool kit that can easily provide APIs (application programming interface) for integration with others as well as provide APIs for data integration and data sharing with other health sectors, MoHP and WHO.
Nursing Association of Nepal (NAN) sent nurse teams to affected areas such as: Sindhupalchowk (Thulobhotang, Chautara, Melamchi), Jiri, Dhading, Nuwakot, Sankhu, Bhaktapur, Harishiddhi, Sitapaila, Ramkot, Macchegaon, and White Gumba to bring medicine, rice, food, clothes, water, soup and distributed these to the affected areas.
The study drew on a combination of quantitative and qualitative data supported by case study. Traditional paper and telephone method for data collection took more time than the smartphone application due to accessibility. To solve this problem, we developed new application collaborated with the local NPO and company. As a result, it enables communication in real time and supplies relevant information. The mobile application collected data and shelter information such as location and timestamps, geo-tagged photos, and specific questionnaire with location information by the geotagging function. The Cloud service works as a one-stop platform at which all of the data and information of the epidemiological data can be accessed. The Cloud infrastructure with flexible extensibility, within the provided financial resources and further development and expansion along social change, should be used. This system development and action engagement process was designed to engage local nurse in the quality improvement process.
Through engaging practitioners in research, care improved, the quality of reporting changed, nurses response flexibly and nursing association was provided with information. This study showed that identifying shared information and engaging domestic community nurses and stakeholders in practical activity to achieve this goal can bring about sustained community health improvement. The government and donor who supported and guided the study as partners now have a basis to apply reconstruction of the results. They are closer to their goals of consolidating data into one database where data can be analyzed automatically. Meanwhile, this study shows the needs for domestic health professionals like community health nurses to take urgent steps to make available information more intelligible and develop a sustainable network to ensure that no one is left behind in disaster risk reduction.
Initially, there was a relatively low commitment among the participating local nurses to continuous monitoring. But the use of Apps increased the health professionals’ sense of responsibility towards the care they provided. To change societal behavior reforms in institutional policies and procedures must co-evolve with health environment changes related to people’s beliefs, norms and values that provide a motivating force for a particular type of behavior.
Conclusion
1) Routine health security monitoring and emergency report based on public health: Resources are often limited and do not allow monitoring tool to incorporate all of the reporting sources. It is required for government to coordinate the interoperability of rapid assessment with other data services for further cooperation with other sectors, such as infrastructure, energy, transport, and water, and close partnerships with local volunteer. These team responsible for rapid assessing each emergency should exist in sustainable community for health security. Routine monitoring and communication is essential in ensuring to adapt over time to changing social context, environments systems and technology. At a minimum communication and regular social capital evaluation should be undertaken. This trajectory may later result in a mode of transferring guidance to first responders and civilian populations regarding DRR and behavior and also as a way to reach large populations.
2) Capacity building including human and technology in sustainable community: With formal education and drilling as well as ICT utility, competency can be developed in public health. It may enable for local nurses to make decision to create a system that would allow smooth cooperation among stakeholders. In local communities, nurses collect information about and mitigate communicable diseases risks. Effective leadership might be also necessary to manage improvement in reconstruction settings. By position, being member of every part of the health care system, they can become critically needed leaders in emergency management and disaster preparedness. Nurses may manage community setting as well as hospital ward. They can play vital role in restoration of public health under disaster condition (water, sanitation, food, and shelter) and identification of high risk and vulnerable population including unique needs of children in disaster.
This project has explored how the data collected by local nurses could become the basis of the daily community health information system, which could the monitoring model and benchmark of Nepal toward SFDRR from the point of view of nursing science. The Nepali local nurses gather first-hand information from evacuees in shelters and transmit data in near real-time communication to other health organizations, who would make informed decisions for prevention of communicable diseases before an outbreak, and enhance organizational development through teamwork around data collection, and to improve the quality of care by linking community and government surveillance records.
Acknowledgement: This project was funded by Japan-Nepal Urgent Collaborative Projects Regarding the April 2015 Nepal Earthquake within the J-RAPID Program